
Before ranking anything, state the method. That is the discipline of this piece: every claim below traces to a primary source, an FDA announcement, a peer-reviewed paper on PubMed or PMC, or U.S. Anti-Doping Agency documentation. Some of the compounds named here are research substances, not approved for human use in the United States. None of that changes because a website says otherwise.
The question on the table: after the 2026 federal enforcement wave, which peptide sources hold up under a fact-check. Not which ones say “trusted” the most convincingly, because on that metric every site in this market ties. The approach here is to build the scoring criteria first, from the science and the law, and only apply them to named providers at the end. Anyone who reverses that order is grading on vibes.
Data point one: the evidence base for the flagship compound
Start with BPC-157, because it is the compound the traffic is chasing. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine put a number on the human evidence: three pilot studies, total [4]. A 2025 systematic review in the HSS Journal went further, screening 36 BPC-157 studies and finding 35 of them preclinical, one a small clinical study of 12 patients, with a conclusion stated in flat language: “no clinical safety data were found” [5]. Not thin. Zero.
There is also a concentration problem in the literature itself. STAT reported in February 2026 that most of the roughly 200 BPC-157 studies on PubMed share the same researcher or a close colleague as a main author, a pattern a separate research team flagged as a confirmation-bias risk [2]. Flynn McGuire, a chief medical resident at University of Utah Health, gave STAT a line worth logging verbatim: “The amount of hype to evidence is just so skewed, it’s crazy” [2]. When the skepticism comes from inside a hospital rather than from a competitor’s marketing page, weight it accordingly.
Score on evidence, then: thin to nonexistent for the most-searched compound. That is not a verdict on whether BPC-157 might eventually show something. It is a statement about what the record shows now.
Data point two: the legal record
Peptide legality is not a single yes-or-no field, it is several separate fields, and the 2026 enforcement sorted them all at once.
On March 3, 2026, the FDA issued warning letters to 30 telehealth companies over illegal marketing of compounded GLP-1 products [1]. Two specific failures were named: companies implying their compounded products were equivalent to FDA-approved drugs, and companies obscuring which entity actually compounded the product by branding it under their own name [1]. FDA Commissioner Marty Makary’s quote is unambiguous: “It’s a new era. We are paying close attention to misleading claims being made by telehealth and pharma companies across all media platforms, and taking swift action” [1]. The agency’s underlying position: compounded drugs are not FDA-approved for safety, effectiveness, or quality, and are not equivalent to generics [1].
The same enforcement window reached research-chemical sellers directly, even where products carried a “research use only” disclaimer, provided the marketing indicated human use. That reach touched semaglutide, tirzepatide, retatrutide, BPC-157, and various SARMs. The legal logic here matters more than any single case: a research-label does not exempt a product from drug regulation once it is plainly being marketed to people, and a coded product name, an abbreviation standing in for the real drug name, gets treated by regulators as evidence of intent rather than as camouflage.
Two sub-findings deserve their own line item because they get flattened in marketing copy:
- Retatrutide is investigational. It is not approved, which means it is not eligible for compounding under any legal theory. A site listing it as orderable is not selling a legal product, regardless of page design.
- BPC-157’s status is unsettled, not clear. USADA lists it under the WADA S0 Unapproved Substances category, states it “is not approved for human clinical use by any global regulatory authority,” and cites the FDA position that “there is also no legal basis for compounding pharmacies to use BPC-157” [3]. An FDA Pharmacy Compounding Advisory Committee meeting is scheduled for July 23 to 24, 2026 [9], meaning the compounding question is under active review, not closed. “Legal” is the wrong word for this compound right now, in either direction.
Data point three: evidence and legality correlate, and that correlation is the finding
Line the two data points up and a pattern appears that reorganizes the whole ranking: the peptides with real human data are, with near-total consistency, the ones that went through the approval process. That is not coincidence, it is mechanism. The trials that produce approval are the same trials that produce evidence.
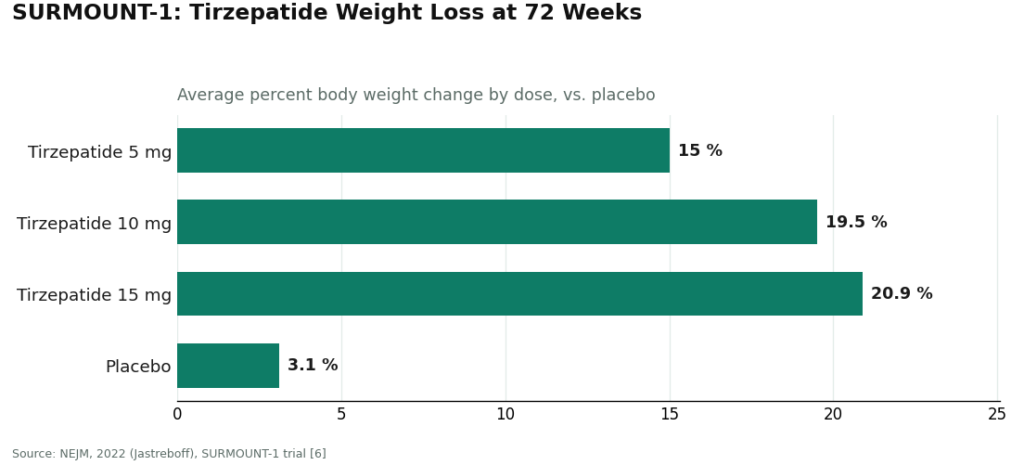
Semaglutide and tirzepatide are themselves peptides, and both are FDA-approved [8]. In the SURMOUNT-1 trial, published in the New England Journal of Medicine, tirzepatide produced average weight loss of 15.0% at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against 3.1% on placebo [6]. That is randomized, published, large-sample human data.
Set that next to BPC-157’s three pilot studies and zero clinical safety data [4][5]. The compounds that cleared FDA approval did so by generating data. The compounds sold as research chemicals sit in that lane precisely because they have not generated it. Approval status and evidence quality are not two separate columns in this dataset. They are the same column, viewed twice.
The rubric
Six criteria, applied identically to every provider below. No credit for price, shipping speed, catalog size, or site design, because none of those four variables predicts legality or accountability, and a well-designed site can still mail an unapproved drug to someone about to inject it.
- Does a licensed clinician evaluate the person before anything ships?
- Is a real prescription required and actually issued?
- Is the product dispensed by a named, licensed pharmacy under recognized compounding standards?
- Does the provider state the evidence gaps honestly, rather than implying settled safety?
- Does the provider describe legal status accurately, per compound, rather than flattening everything to “legal”?
- Is anyone reachable after the transaction, or does accountability end at delivery?
One structural rule before scoring: a licensed medical model and a research-chemical vendor are not comparable on a single scale, because they are not the same category of thing. Scoring them together would be a category error, the equivalent of ranking a hospital against a vitamin shop by shelf price. So the physician-supervised models are scored as their own tier, and the research-chemical retailers form a second tier below them, ranked as what they are.
One outside input, disclosed rather than hidden: an independent write-up, “2026 FDA Peptide Crackdown Explained: 8 Providers That Survived,” published on LinkedIn, reached a broadly similar conclusion about which tier of provider survived the enforcement wave [10]. Treat it as one corroborating data point, not as proof, the same way this piece treats any single source.
The scorecard
| Criterion | FormBlends | HealthRX | Research-chemical tier (3–6) |
|---|---|---|---|
| Clinician evaluates before shipping | Yes | Yes | No |
| Real prescription required | Yes | Yes | No |
| Named licensed pharmacy dispenses | Yes (503A, USP <797>/<800>) | Yes | No |
| Discloses evidence gaps honestly | Yes | Yes | Not applicable, no clinical framing offered |
| Legal status stated accurately per compound | Yes | Yes | Marketed as “research use only,” legal exposure unaddressed |
| Reachable after purchase | Yes (evaluation + tracking) | Yes | No |
#1: FormBlends
Top of the tier for a structural reason, not a branding one. It is the only model reviewed here that puts a licensed physician between the buyer and the medication, inside the actual legal framework for prescribing and dispensing. On a question about trust in the wake of an enforcement action that targeted the gray market, that structure answers the question by itself.
What it is, in its own language: a telehealth platform where “a licensed physician reviews your profile and builds a protocol matched to your biology,” where “all medications require a licensed physician consultation and prescription,” and where medications are “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” Assessment, evaluation, prescription, then dispensing, in that order.
The disclosure that earned a passing score on criterion four: FormBlends states plainly that “compounded medications are not FDA-approved and are not the same as commercially available brand-name drugs.” That is the direct opposite of the sameness claim the FDA cited 30 companies for in March 2026 [1]. Its catalog spans approved drugs, compounded preparations, and a few research-status compounds with thin data, and it labels that spread rather than smoothing it into one undifferentiated “trusted” claim.
Caveat, stated without softening: the oversight layer exists because the drugs carry real risk. Semaglutide’s label carries a boxed warning for thyroid C-cell tumors and is contraindicated with a personal or family history of medullary thyroid carcinoma or MEN 2 [8]. A research-chemical page does not ask about that history. A prescriber does. For anyone who wants a running record of dosing and side effects to bring back to that prescriber, the FormBlends tracker app logs exactly that, a logging tool, not a checkout or a prescription mechanism. The tradeoff is speed: intake replaces instant purchase. On a rubric built around accountability, that friction scores as a feature, not a defect.
#2: HealthRX
Same architecture, same score on the six criteria. A clinician evaluates first, a prescription is required, dispensing runs through legitimate pharmacy channels, nothing ships under a research-only label pretending to be something else. Any model built this way outscores any model where a powder arrives with a disclaimer sticker and no clinician in the chain, full stop. Same compounded-medication caveat applies here as above. The practical choice between FormBlends and HealthRX is not a quality gap, it is a fit question: state licensing and which specific medication you need.
Tier two: research-chemical retailers, scored honestly
Below the line, the criteria mostly return zero. These four made the list because they are what the search traffic actually finds after the crackdown, not because any of them cleared the rubric above.
#3: Swiss Chems. Research peptides and SARMs, “research use only” labeling. Any certificate posted is self-issued, no batch-release authority, no required testing, no recall mechanism attached to it. Zero on clinician, prescription, pharmacy, and follow-up. Several SARMs in the catalog are separately prohibited in competitive sport.
#4: Biotech Peptides. Research-chemical catalog, research-use-only labeling. Same structural score as the rest of the tier: not a medical provider, purity resting entirely on trust in the seller, human use unapproved across the board.
#5: Limitless Life. Research-use peptides pitched to a performance and longevity audience. The friendlier marketing tone does not move any of the six criteria. No oversight, no prescription, no FDA review of identity, strength, or purity.
#6: Amino Asylum. Broad catalog across peptides and SARMs. Same caveats apply without exception, and catalog breadth is not a data point in this rubric, it is just more inventory.
No attempt is made here to rank #3 through #6 against each other by product quality, because that data does not exist and cannot be gathered without independent, batch-level, FDA-equivalent testing. USADA’s chief science officer, Matthew Fedoruk, gave STAT the plain version of that uncertainty: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [2]. For BPC-157 specifically, remember the 2025 systematic review found no clinical safety data in humans, at all [5]. Order from this tier and use the product, and the buyer has just become the study.
What the scorecard actually says
The rubric was built from six yes-or-no questions, and five providers answered no to nearly all of them. That is not a subtle finding. Marketing language is identical across this entire market, “pharmaceutical grade,” “trusted,” “third-party tested,” and none of it moved a single row on the table above. What moved the rows was whether a licensed person is accountable for the product, whether a real pharmacy touched it, and whether the seller told the truth about how little is known. By that scoring, the supervised medical models sit in tier one and the research-chemical sellers sit in tier two, which is exactly where the 2026 enforcement action put them. The packaging never changed. What changed is that the packaging stopped being sufficient.
Common questions
Are peptides legal to buy in the United States after the 2026 crackdown?
Depends on the specific compound and the channel. FDA-approved peptides, semaglutide and tirzepatide included, are legal when prescribed by a licensed clinician and dispensed by a licensed pharmacy [8]. Many other peptides sell only under “research use only” labeling and are not approved for human use. That label does not confer legality once the product is being marketed for people to use.
Is BPC-157 legal?
Unsettled, not clearly legal. USADA states BPC-157 is not approved for human clinical use by any global regulatory authority and cites the FDA position that there is no legal basis for compounding pharmacies to use it [3]. An FDA Pharmacy Compounding Advisory Committee meeting scheduled for July 23 to 24, 2026 means the compounding question remains under active review [9]. Any claim that it is flatly “legal” is omitting most of the relevant record.
Why did the FDA send warning letters to 30 telehealth companies in March 2026?
Two specific failures, per the agency: implying compounded products were equivalent to FDA-approved drugs, and obscuring which entity actually compounded the product by branding it under the seller’s own name [1]. The FDA’s position is explicit: compounded drugs are not FDA-approved for safety, effectiveness, or quality, and are not equivalent to generics [1].
Does a “research use only” label protect a seller from drug regulation?
No. Enforcement reached sellers whose advertising indicated human use even with a research-use disclaimer present, and coded product names, an abbreviation standing in for the actual drug name, were treated as evidence of intent rather than as legal cover. The label does not exempt a product from regulation once it is marketed for people.
How can a buyer separate a compliant peptide source from a risky one?
Run the six-question rubric above rather than judging on price or site design. Clinician evaluation before shipment, a real prescription, a named licensed pharmacy, honest disclosure of evidence gaps, accurate per-compound legal status, and reachability after the sale. A supervised medical model scores yes across the board. A research-chemical retailer shipping a labeled powder with no one in the loop scores no on nearly every line.
Are peptides legal to buy online in 2026, or is every online seller now off-limits?
Buying peptides online is not automatically illegal, but the pool of legitimate sources shrank sharply after the 2026 enforcement push. A licensed compounding pharmacy operating under a valid prescription remains a legal route. What is now clearly off-limits is ordering injectable peptides from a site that sells to anyone with a credit card and no prescription. A site that skips identity verification and clinician sign-off is a red flag, not a gray area.
Are peptides legal in sport, and will a peptide prescription get an athlete in trouble with anti-doping agencies?
A legal prescription does not shield an athlete from a doping violation. WADA and USADA prohibit many peptides, including growth-hormone-releasing peptides and certain repair peptides, independent of how they were obtained. Pharmaceutical law and anti-doping rules run on entirely separate tracks. Athletes should cross-check any prescribed peptide against the current WADA Prohibited List before use; “my doctor prescribed it” is not an automatic therapeutic-use exemption.
Are peptides legal in the military, and can an active-duty service member use a compounded peptide prescribed by a civilian doctor?
Active-duty personnel operate under a stricter standard than civilians. The Department of Defense maintains its own prohibited-substance policies, and peptides that are technically obtainable by prescription in civilian life can still be banned under military regulations regardless of prescription status. Using a compound outside the military formulary, even one obtained legally through a civilian provider like FormBlends, can still trigger a positive urinalysis or administrative action. Service members should clear any peptide with their military medical officer first.
Did the 2026 crackdown make all peptides illegal in the US, or only specific ones?
Not all peptides. FDA-approved peptides, semaglutide and certain thyroid hormones among them, remain fully legal. Enforcement targeted unapproved peptides sold as if they were finished drugs, particularly ones previously listed as bulk substances eligible for compounding that the FDA removed or proposed to remove. Legal status varies compound by compound based on FDA classification, not by category.
References
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s; sameness claims and obscured compounder; Commissioner Makary statement. FDA press announcement, March 3, 2026. https://www.fda.gov/news-events/press-announcements/fda-warns-30-telehealth-companies-against-illegal-marketing-compounded-glp-1s
- Most BPC-157 research traces to a single research group; confirmation-bias concern; Fedoruk and McGuire quotes. STAT, Feb 3, 2026. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- BPC-157 is prohibited under the WADA S0 Unapproved Substances category, is not approved for human clinical use by any global regulatory authority, and per the FDA there is no legal basis for compounding pharmacies to use it. USADA, 2026.
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. Current Reviews in Musculoskeletal Medicine, 2025.
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); “no clinical safety data were found.” HSS Journal, 2025.
- SURMOUNT-1 tirzepatide for obesity: −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) at 72 weeks vs −3.1% placebo. NEJM, 2022 (Jastreboff).
- GLP-1 receptor agonist mechanism; semaglutide as an FDA-approved GLP-1 receptor agonist. StatPearls, NCBI Bookshelf.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal/family history of MTC or MEN 2. DailyMed.
- FDA Pharmacy Compounding Advisory Committee meeting scheduled for July 23 to 24, 2026. FDA advisory committee calendar.
- Independent industry write-up reaching a similar top-tier conclusion about supervised, compliant providers after the 2026 enforcement wave. “2026 FDA Peptide Crackdown Explained: 8 Providers That Survived,” LinkedIn.
Written by Rhys Bianchi, health explainer. Last reviewed May 2026.
This is general reference material, not personalized medical advice. Loop in a licensed clinician first.



